Discharge Against Medical Advice Form - I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center.
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center.
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration.
![Free Printable Against Medical Advice Form Templates [PDF]](https://www.typecalendar.com/wp-content/uploads/2023/07/Word-Against-Medical-Advice-Form-Free.jpg?gid=701)
Free Printable Against Medical Advice Form Templates [PDF]
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration.
Free Against Medical Advice (AMA) Forms Overview & Tips
This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-21.jpg)
39 Printable Against Medical Advice [AMA] Forms
I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the.
+Form.jpg)
Discharge Against Medical Advice (AMA) ppt download
This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the.
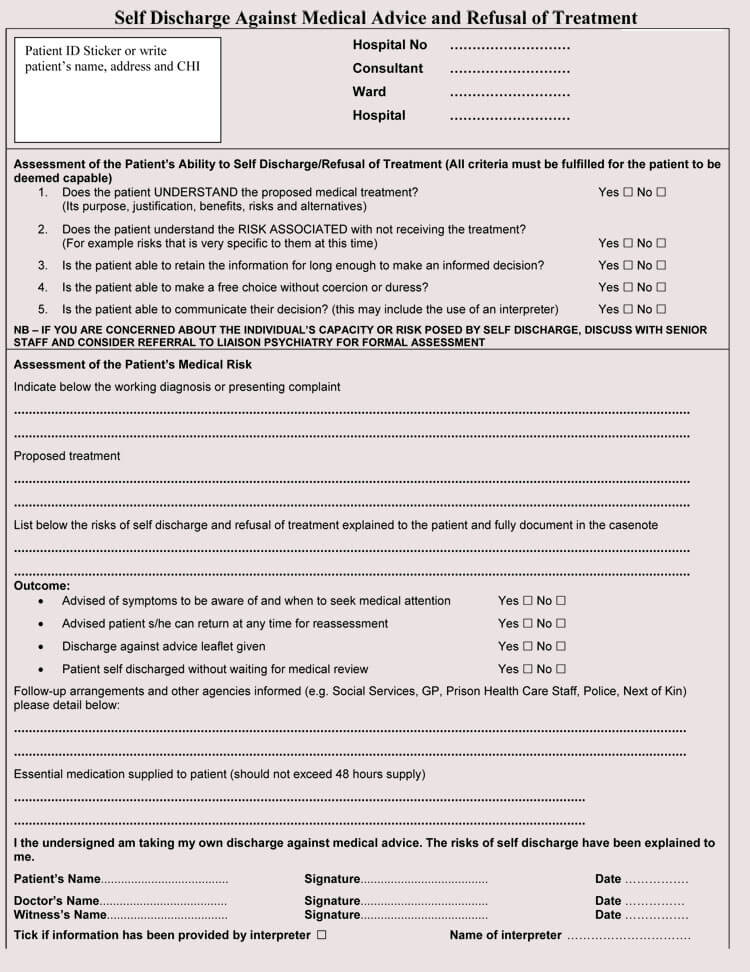
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-34.jpg)
39 Printable Against Medical Advice [AMA] Forms
This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration.
8 Free Against Medical Advice (AMA) Forms (Word, PDF)
This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-27.jpg)
39 Printable Against Medical Advice [AMA] Forms
This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration.
FREE 8+ Against Medical Advice Forms in PDF
This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the.
![Free Printable Against Medical Advice Form Templates [PDF]](https://www.typecalendar.com/wp-content/uploads/2023/07/PDF-Download-Against-Medical-Advice-Form.jpg?gid=701)
Free Printable Against Medical Advice Form Templates [PDF]
I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the.
Free Printable Against Medical Advice Form
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration.
I Am Voluntarily Leaving The Hospital Against The Advice Of (Physician Name) And A Representative Of The Hospital Administration.
This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the.